Estimated readtime: 5.5 min
Authors: Priscilla Rouyer, Dr. Sebastian Ilomuanya (CHAI Global Vaccines Delivery), Jon Robertson (Vaccines Programme Manager, CHAI Sierra Leone), and Dr. Tom Sesay (CH/EPI Programme Manager, Government of Sierra Leone)
The COVID-19 pandemic has caused major disruptions to the provision of health care services. Initial estimates and modeling analysis show the potential magnitude of these disruptions, with a recent study funded by the Bill and Melinda Gates Foundation in 118 low-and middle-income countries estimating that up to 1.1 million additional children and 56,000 additional mothers have died since March due to the ripple effects of these interruptions to health services[1]. National immunization programs are no exception. Disruptions related to lockdown measures, transport restrictions, and reduced demand due to fear or mistrust have affected vaccine coverage with most countries reporting a 6 to 12 percent decrease over the past few months[2]. This has increased the burden on programs across healthcare systems who are faced with complex challenges: how to balance the response to COVID-19 while ensuring the continued delivery of immunization services? how to allocate scarce resources even as the need for those resources rises? and amidst these resource constraints, what trade-offs to make?
In Sierra Leone, the Expanded Program for Immunization (EPI), which is responsible for reducing the burden of vaccine-preventable diseases through childhood immunization services, is facing these challenges. Difficult decisions need to be made on where to prioritize services, based not only on pre-existing shortages but also on those hard hit by COVID-19 restrictions. To make these decisions, the program needs to know vaccine coverage, stock availability, implementation rates of planned activities, and services across the districts. In addition to the data, tools are needed to analyze available information, identify trends, and build a case for policymakers to invest in and prioritize immunization services amidst the pandemic.
Over the past few months, the Clinton Health Access Initiative (CHAI) together with the EPI program has developed an Excel-based tracker designed to evaluate the impact of COVID-19 across the country, and inform decisions regarding catch-up plans and allocation of resources.
Effective data management and review meetings key for equitable distribution of resources during COVID-19
Sierra Leone does not have a single, comprehensive database that hosts all of the country’s health-related data for easy extraction and analysis by data specialists in government. The EPI still uses paper forms and spreadsheets at all levels of government despite advances in electronic health information management and logistics management systems. However, things are gradually beginning to improve thanks to a concerted effort on data strengthening by the program.
Until last year, the program had to consult individual paper reports from each of the fourteen districts to understand and compare vaccine stock levels at each facility. The data was often late, patchy, and difficult to combine and analyze. The pandemic only made this process more difficult due to lockdowns and social distancing policies.
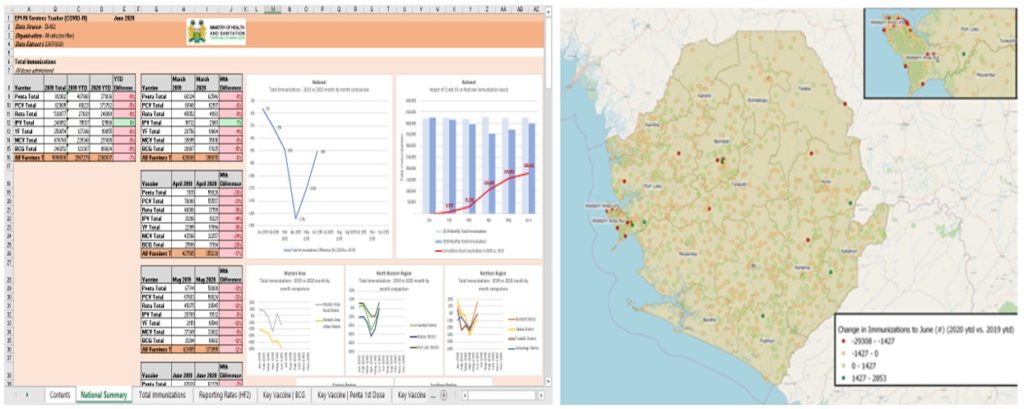
In response, the CHAI Sierra Leone team worked with the EPI program to develop an Excel-based tracker specifically designed to track the impact of COVID-19 across the country at national, district, and facility levels, using the information collected in the District Health Information Software 2 (DHIS2). The tracker monitors the percentage change in immunizations between similar antigens at two comparable periods. Together with open-source geospatial mapping software, the tracker is used to visualize and identify areas heavily impacted by COVID-19, and to prioritize resource allocation there.
Conducting productive review meetings amid the pandemic
While the dashboard and maps are helping the EPI mount an adequate response to the pandemic, new rules around social distancing and limits on in-person gatherings mean that EPI management needs to come up with creative workarounds to review the newly available data and make decisions with key partners.
CHAI worked with the program to establish virtual data review meetings with four focus districts. For two hours each month, members of EPI’s management team, CHAI, district officers, and managers meet via videoconference to systematically review stock out trends, rank immunization performance compared to historical averages, and assess data quality from facilities. The meetings consider the technical, programmatic, and management requirements for a successful virtual review meeting (Figure 2).

To kick start these meetings, CHAI conducted a virtual training for the district officers via the WhatsApp platform on how to download and use the Zoom and Google Drive accounts created for the meetings and data storage respectively. The WhatsApp platform also served as the medium for disseminating information and reminders at least a day before the meeting, providing feedback and other crucial updates.
These meetings, which are facilitated by the EPI and supported by CHAI, are aimed at reviewing district performance and trends, which are measured against a set of key performance indicators (KPIs)[3], identifying causes and implications, and delegating follow-up actions captured by the EPI team. During the meeting, action items are assigned to specific team members with timelines to complete the activity and provide feedback, enabling progress to be tracked and reviewed.
This is notwithstanding certain challenges such as internet downtime and keeping to a regular meeting frequency, considering government competing priorities. Resolving these two challenges requires flexibility in scheduling and exploring backup internet subscriptions on other platforms. To mitigate connectivity challenges, CHAI deployed six Mifis[4] with unlimited data subscriptions and had backup Mifis to be used in the event of internet downtime. This strategy has proved effective as the team has rarely encountered a situation where all available networks experienced downtime simultaneously.
These data reviews facilitated through monthly videoconferencing have led to higher reporting rates of stock information in DHIS2 by facilities in the supported districts, showing a reporting increase from 84 percent to 96 percent between April and September. Monthly stock out and data quality issues were also addressed through targeted coaching of health facilities by the program. Three of the four districts supported with monthly videoconferencing managed to recover to greater than 2019 levels of monthly routine immunizations less than three months after the worst of the crisis in April. By August 2020, the fourth supported district had also recovered to greater than 2019 levels of monthly immunizations.
What are we taking away from this experience?
An unexpected benefit from the data review videoconferencing is that the meetings have permitted the Sierra Leone EPI national program to be more connected to the district health management teams, resulting in better coordination and effective delivery of immunization services. Furthermore, they have enabled the program to recognize and acknowledge effective district health management performance and resolve common problems across the districts, better and faster. And this, the program hopes, is a key lesson for other health programs in the country and elsewhere.
This blog was co-authored by Priscilla Rouyer, Dr. Sebastian Ilomuanya (CHAI Global Vaccines Delivery), Jon Robertson (Vaccines Programme Manager, CHAI Sierra Leone), and Dr. Tom Sesay (CH/EPI Programme Manager, Government of Sierra Leone). We would also like to acknowledge the contributions of Rumbidzai Ndungwani and Michael Jones (CHAI Sierra Leone) towards the implementation of the work reported here.
[1] https://www.thelancet.com/pdfs/journals/langlo/PIIS2214-109X(20)30229-1.pdf
[2]Gavi (2020). COVID-19 Situation Report #10, Gavi, the Vaccine Alliance, 2 June 2020 https://www.gavi.org/sites/default/files/document/2020/Gavi-COVID-19-Situation-Report-10-20200602.pdf
[3] KPIs measured include reporting rate, facility stock outs, data quality, and vaccine wastage.
[4] A mobile Wi-Fi device